

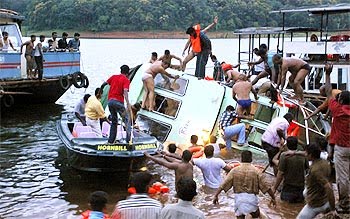
The accident happened when the boat "Jalakanyaka" tilted after several tourists moved to one side on sighting elephants on the banks of the lake and the driver lost control. This happened around sunset making rescue operations dfficult. It was shocking to note that none of the passen gers were wearing life jackets and there were no prior instructions to passengers on safety aspects by the boat crew before the journey. Also there were no life guards in the boat.
Drowning means death due to suffocation with or without aspiration of water while submerged in water.Near drowning means suffocation and asphyxia but with possible survival. Asphyxia due to submersion or hypoxia due to aspiration of water or a combination of both occur in drowning leading to death. Drowning can be either fresh water (well, lakes) or sea water.Also classified as dry or wet drowning. In dry drowning the victim is subjected to severe reflex laryngospasm and hypoxia following accidental contact with cold water and death is primarily due to asphyxia ( lungs are free of water). In wet drowning water enters the lung and cause alveolar flooding, alveolar edema, loss of surfactant, ventilation perfusion mismatch ,bronchospasm and hypoxia. Disruption of the alveolocapillary membranes lead on to ARDS.
In fresh water drowning the hypotonic water aspirated is rapidly absorbed into the pulmonary circulation an amount of more than 500-800 ml can cause hemodilution, hyponatremia and hemolysis. In salt water drowning water is drawn into the alveoli from pulmonary circulation causing hemoconcentration and hypernatremia.Hypermagnesemia and hypercalcemia are also seen in salt water drowning The patient may lose consciousness in cold water drowning if body temperature is below 32 deg.C.Ventricular fibrillation may occur. It is stated that hypothermia has protective effects on brain and favourable neurological outcome following successful resuscitation is possible.
Clinical manifestations: Patients present with hypoxia, hypercarbia and metabolic acidosis.Injury to cerv ical spines to be considered in divers or in victims of "water accidents" The recovery may be complicated by permanent neurologic sequealae or ARDS.
Emergency management:
- Call for help emergency response system
- The victim should be removed from the water early as possible with attention to cervical spine
- Open the mouth and clear the airway of mud, weed, other foreign bodies or vomitus using finger sweep technique.Rescue breathing should be performed while the individual is still in water, or on board in a boat.But chest compressions are inadequate because of buoyancy issues.. Do not attempt to deliver abdominal thrusts to expel water as it can cause aspiration of water or induce vomiting.
- Alternately bag and mask ventilation using 100% oxygen with airway and cricoid pressure can also be performed if resuscitation equipments are available nearby.
- Cardiac compressions shoul be initiated. Advanced cardiac Life support by intubation and drugs to be followed, if the victim is still unresponsive.
In hospital management:
Immediate rewarming measures initiated to prevent ventricular fibrillation if body temperature is below 25 deg. Hypothermia improves neurological oucome so rapid rewarming to room temperature is to be avoided if body temp is above 30 deg and patient is hypoxic. Core rewaming can be performed with warm oxygen, continuous bladder lavage with fluid at 40°C, and intravenous (IV) infusion of isotonic fluids at 40°C and warm fluids through Ryles tube.
Recent investigations In 2002, by the American Heart Association, followed in 2003 by the European Resuscitation Council, based on the results of blinded, randomized, multicenter clinical trials, suggest induced hypothermia(Therapeutic hypothermia (TH)) improves oxygen supply to ischemic brain areas, decreases cerebral metabolic demand, and decreases increased intracranial pressure.But the danger of hypoperfusion, acidosis and cardiac complications of hypothermia are also to be considered.
Intubation may be required in order to provide adequate oxygenationif 100% oxygen by face mask is ineffective to maintain oxygenation.Protect the cervical spines in cervical collar or apply manual in line traction during intubation. Criteria for ET intubation include the following:
- PO2 less than 60-70 mm Hg (>80 mm Hg in children) on 100% oxygen by mask
- Impaired consciousness and inability to protect airway or handle secretions
- High alveolar-arterial (A-a) gradient - PaO2 of 60-80 mm Hg or less on 15 L oxygen by non rebreathing mask
- Respiratory failure - PaCO2 >45 mm Hg
- Unsatisfactory ABG results
- Shifting interstitial water into the pulmonary capillaries,
- Prevention of alveolar collapse,
- Adequate alveolar ventilation and decreasing capillary permeability and
- Increasing the diameter of both small and large airways to improve distribution of ventilation.
Thoracotomy with open heart massage and warm mediastinal lavage may be required in selected patients as the hypothermic heart is typically unresponsive to pharmacotherapy ,cardioversion or defibrillation
Extracorporeal blood rewarming may be considered in severe hypothermia unresponsive to above measures. Do not abandon resuscitation of a submersion victim until the patient has been warmed to a minimum of 30°C because of the reasons mentioned above
Other treaments include:
- Beta 2 agonists as Nebulization Albuterol 1.25-2.5 mg diluted in 2-5 mL sterile saline or water Q8
- Inotropic support dopamine 10-20 mic/kg/mt
- Treatment of hemolysis by blood transfusion
- Correction of electrolyte abnormalities
- Antibiotic therapy
- Decompression of stomach using ryles tube
- Raised intracranial tension management according to protocols
- Ventilatory management of ARDS
- Children, especially toddlers, should be under supervision when they are around water, including a bathtub or bucket full of water.
- All individuals involved in boating activities water sports or recreational activities in beach should be able to swim, and should wear life jackets while onboard
- Avoid alcohol or drugs while boating or swimming
- Individuals with underlying medical illnesses such as seizure disorder, diabetes mellitus,or coronary artery disease, should swim only under supervision
- All tourists should make sure that boating facilities are provided by an authorised authority.Thet should see whether adequate life saving equipments including life jackets and trained rescuers are available while boating
Ref: Article on Drowning from emedicine medscape; by Suzanne Moore Shepherd, MD, William H Shoff, MD, Professors, Department of Emergency Medicine, Hospital of the University of Pennsylvania;
http://emedicine.medscape.com/article/772753-overview
Oxford Handbook of Critical Care 3rd edition
Clinical Anaesthesiology, Morgan, Mikhail, third edition, Mc Graw Hill













No comments:
Post a Comment